- Visibility 33 Views
- Downloads 7 Downloads
- DOI 10.18231/j.ijos.2020.009
-
CrossMark

Transient quadriparesis without bony injury in overhead weight carrying labourers-cervical cord concussion—Myelopraxia
Introduction
The cervical spinal cord may be damaged by a variety of factors associated with or without frank fracture, fracture dislocation of cervical vertebrae along with neurological weakness quadriparesis or quadriplegia with bowel and bladder involvement. The diagnosis is often clear on roentgenogram when it is associated with fracture or fracture dislocation of cervical vertebra. But it is difficult to diagnose a patient having cervical spine injury with history of neurological weakness and the roentgenograms appear apparently normal. Nevertheless the diagnosis is still often overlooked on initial examination.
This type of cervical spinal cord injury with transient quadriparesis without apparent bony injury is discussed in overhead heavy weight carrying laborers. This injury is quite similar to acute central cord syndrome without bony injury.
Mode of Injury
We have come across such type of cervical spinal cord injury occurring in these overhead load carrying labourers and farmers in our region carrying heaps of grass and sugarcane bundles over head. These labourers carry heavy bundles overhead from one place to another place in their farms to load and unload them in tractors or trucks or bullock carts. These labourers often sustained cervical spinal cord injury and got admitted in the hospital for transient quadriparesis.
Majority of the patients admitted had a history of carrying heavy weight bundles of sugarcane or grass bundles. The ages of these patients ranged between fifty two to sixty five years. All were males. The bundles are placed overhead longitudinally in the sagittal plane of body. To avoid the obstruction of vision by overhanging sugarcane or grass bundles, they had to hyper extend the neck to have unobstructed view to walk ahead ([Figure 1]).
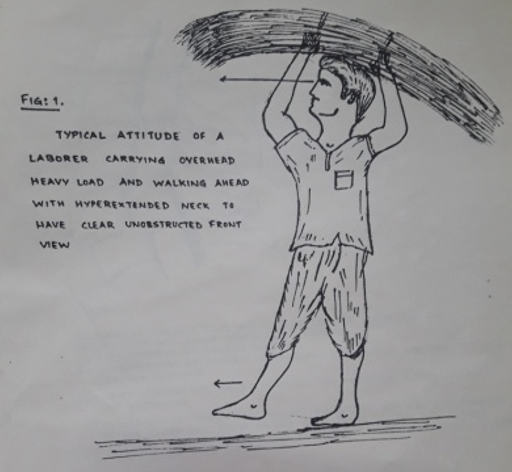
After reaching the destination they throw the overhead load suddenly on to the ground or tractor or bullockcart by hyperextending the neck followed by full flexion of cervical spine for deloading the overhead weight. The moment they drop the overhead load on to the ground they noticed sudden loss of power in both upper and lower limbs associated with tingling and numbness and neck pain and fall helplessly on the ground. They were then carried by their friends or relatives to the hospital.
Case Report
We had encountered seven patients. All were male aged between 48 to 65 yrs. Six patients were farmers and one was coolie. We noted their history and mechanism of injury. Clinical assessment of patient was done with specific focus on neurological examination. There was broad spectrum of neurological deficit ranging from mild and transient symptoms such as tingling and numbness, parasthesia in fingers to quadriparesis. In two of cases the neurological symptoms became apparent after 2 to 3 days of injury. Conventional X-rays of cervical spine AP and lateral views was performed as first line imaging test. Diagnostic test is MRI which can show important prognostic factors like small haematoma or cord oedema which have favourable prognosis and resolve in most of the cases. Larger sized haematoma greater than half of spinal cord diameter have poor prognosis. We did not include those patients in our study who had obvious cervical spine fracture or fracture dislocations on X-ray.
A fifty five years male was admitted in our hospital with history of neck pain, tingling and numbness with associated weakness in both upper and lower limb. On detailed enquiry of history mode of injury revealed classical pattern as described above.
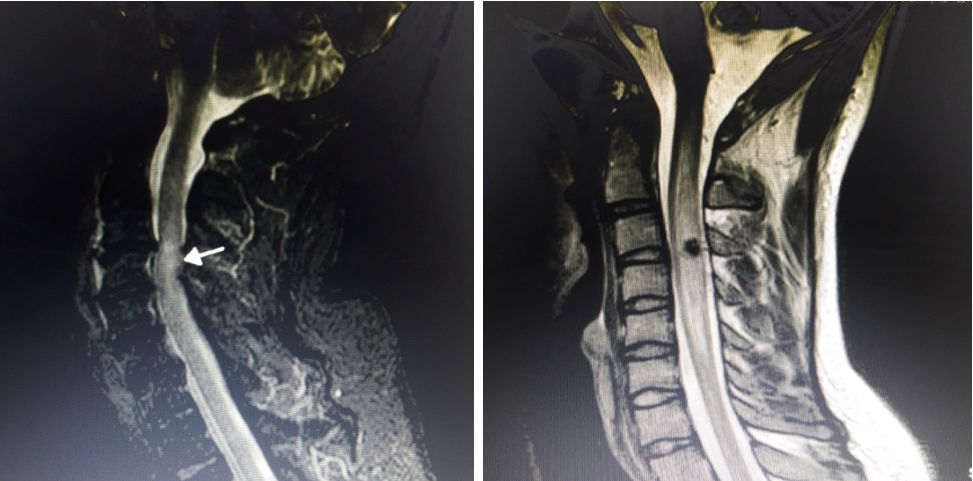
He was brought to the hospital by his relatives. The latent period from time of injury to time of admission was about 6 to 8 hours. On examination we found cervical spine tenderness, paraspinal muscle spasm, and restricted movements at neck. Neurological examination revealed weakness in all four limbs more so in upper limb about grade three and four. There was no bladder and bowel involvement. Sensations were well preserved. Deep tendon reflexes were normal. X-rays of cervical spine AP and Lateral views were found to be apparently normal. His MRI of cervical spine showed moderate cord oedema and small haematoma [Figure 2]. Neurosurgeon opinion was obtained.
Treatment consisted of head halters traction 2-3 kgs for immobilization of cervical spine, a bolous of intravenous steroid tapering over five days. IV fluids on admission and Analgesics and physiotherapy of gradual active assisted movements of all joints were started and motivated. A close observation was done on any deterioration of neurological status and recovery status assessing the tone power reflexes and sensations clinically and was charted on case sheet daily. Patient recovered completely symptomatically as well as neurologically over a period of 12-15 days. Patient was discharged after fifteen days with cervical collar analgesics and was advised to follow up and was advised to not to carry overhead weights henceforth.
Discussion
The first case of SCIWORA was reported by Burke in 1974.[3], [2] The mechanism and pathology of cervical spinal cord injury resulting in to central cord syndrome is well known. This was originally described by Schneider et al[4] in 1954 and is caused by hyper extension of cervical spine associated with or without fracture dislocation and neurological weakness in all four limbs. This syndrome is often seen in patients having degenerative changes of cervical spondylosis
Crook and Birkett (1944) first described the association between cervical spondylosis and spinal cord injury.[1], [5] Barnes 1948 stated that injury to arthritic spine was the usual cause of quadriplegia in patients over fifty years of age. He also stated that compensatory cervical lordosis secondary to senile thyoracic kyphosis resulted into relatively fixed cervical spine with little extension reserve. As a result in patients in which mobility of spine was impaired, any degree of extension was liable to cause cord injury by impingement.[1], [6] The mechanism of cervical spinal cord injury in an intact cervical spine was investigated by Taylor (1951) who demonstrated by myelography in cadavers that when cervical spine was hyperextended the cord was compressed posteriorly by infolding of the ligamentum flavum[8], [7] ([Figure 3]).

In patients having early or late arthritic changes further compression occurred anteriorly by osteophytes resulting in the cord being squeezed between the two. Schneider and Crossby (1959) reported that acute or chronic compression of anterior spinal artery resulted into softening of central portion of cord- myelomalacia and compression of vertebral artery, the major feeding vessel of cervical portion of anterior spinal artery results into syringomyelic lesion.[11], [10], [9] It is also possible that stretching of anterior spinal artery during hyperextension of neck causes transient ischemia of the cord resulting in changes found in central cord syndrome.
Concussion or contusion of spinal cord produced by impingement of surrounding structures will be evidenced by uniform swelling of the cord rapidly developing opposite the point of impact. The pathologic changes found to be pronounced oedema in different segments, the most marked involvement being found at the site of blow and extending proximally and distally. In the milder forms of damage the fibres tracts display swollen myelin sheaths and cylinders and the grey matter exhibits small areas of haemorrhagic haematomyelia and neuronal degeneration. Most of these changes are reversible, thereby accounting for neurological deficit that partly or completely disappears as the oedema subsides.[10]
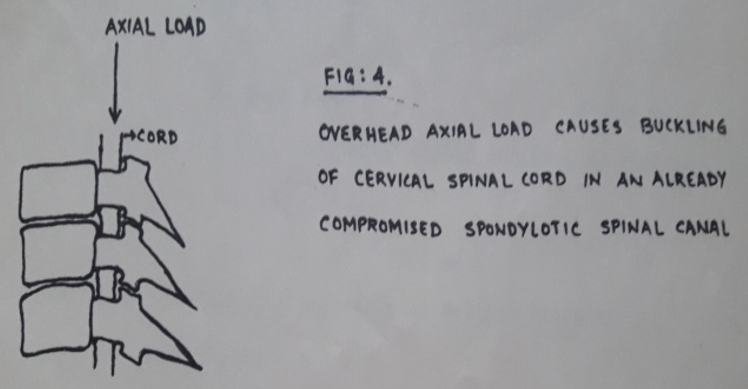
Anatomically the space in the cervical canal accommodating the cervical spinal cord increases in flexion of neck and decreases in extension or hyperextension. This space is further compromised in a spondylotic cervical spine by osteophytes causing pressure over cervical cord. Secondly, when the person carries overhead weight, has to hyperextend the neck to have clear unobstructed front view while walking. This axial load overhead also causes the cervical cord to get buckled up in the already compromised narrow cervical spine canal[4] ([Figure 4]).
Hyperextension trauma in already degenerative cervical spine with added stenosis increases the risk of neuropraxia of cervical spinal cord.
Hyperextension of neck during carrying overhead load for vision clearance and hyperflexion of neck during deloading the overhead load causes stretching of arteries supplying the cervical spinal cord leading to transient ischemia.
Considering the spine factor there are two factors causing cervical spinal cord damage, one of them is bony osteophytes which are anterior to cord and second is soft tissue- infolding of ligamentum flavum posteriorly during hyperextension of neck causing pincer phenomenon squeezing the cervical cord momentarily against the osteophytes and causing transient disruption of cell axonal membrane permeability resulting into reversible depolarisation thus causing quadriparesis. [12] ([Figure 5])
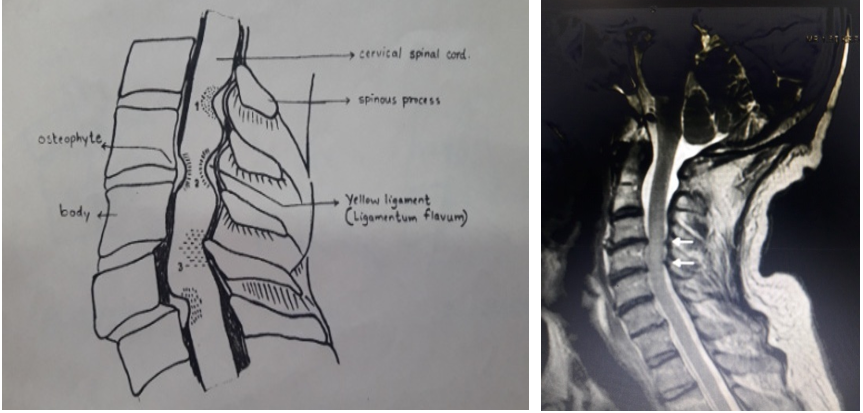
Anatomical factors that may compromise the space for the spinal cord and cause neurologic problems 1) Encroachment by ligamentum flavum posteriorly 2) Encroachment by midline osteophyte anteriorly 3) Pincer phenomenon due to anterior or posterior translation of vertebrae. In all situations cord gets compressed and injured.
This phenomenon of transient quadriparesis due to momentary squeezing of cervical spinal cord leading to temperory physiological conduction block of cord simulates and may be compared with neuropraxia type of peripheral nerve injury and thus may be termed and nomenclated as “MYELOPRAXIA.”
Acknowledgment
I would like to thank Dr Kush Kumar (Formerly Professor and Head Dept. of Orthopaedics KIMS Karad) for his inspiration and guidance.
Source of Funding
None.
Conflict of Interest
None.
References
- G. Holmes. The Goulstonian Lectures ON SPINAL INJURIES OF WARFARE: Delivered before the Royal College of Physicians of London. Br Med J 1915. [Google Scholar]
- D C Burke. Traumatic spinal paralysis in children. Paraplegia 1974. [Google Scholar]
- M J Maxted, G S D Dowd. Acute central cord syndrome without bony injury. injury 1982. [Google Scholar]
- J A Rihn, Andeson, K Lamb, P F Deluca, A Bata, P A Marchetto. Cervical spine injuries in American football. Sports Med 2009. [Google Scholar]
- F. Crooks, A. N. Birkett. Fractures and dislocations of the cervical spine. Br J Surg 1944. [Google Scholar]
- H Barnes. Paraplegia in cervical spine injuries. J Bone Jt Surg 1948. [Google Scholar] [Crossref]
- A R Taylor. The mechanism of injury to spinal cord in the neck without damage to vertebral column. J Bone Jt Surg 1951. [Google Scholar] [Crossref]
- A R Taylor, W Blackwood. Paraplegia in hyperextension cervical injuries with normal radiographic appearancs. J Bone Jt Surg 1948. [Google Scholar]
- Richard C. Schneider, Glenn Cherry, Henry Pantek. The Syndrome of Acute Central Cervical Spinal Cord Injury. J Neurosurg 1954. [Google Scholar] [Crossref]
- R C Schneider, E C Crosby. Vascular insufficiency of brainstem and spinal cord in spinal trauma. Neurol 1959. [Google Scholar]
- R C Schneider, H Cherry G Pantek. The syndrome of acute central cervical spinal cord injury with special reference to mechanism involved in hyperextension injuries. J Neurosurg 1954. [Google Scholar]
- . . Emerg Med J 2002. [Google Scholar]