- Visibility 28 Views
- Downloads 6 Downloads
- DOI 10.18231/j.ijos.2023.005
-
CrossMark

Evaluation of functional and radiological outcome of transverse cancellous lag screw fixation technique in pauwels type 3 fracture neck of femur
- Author Details:
-
 Abhishek Kumar Singh
Abhishek Kumar Singh
-
Gourav Mazumdar *
-
Alif Nidal Vilangil
-
Fazlur Rahmon
Introduction
Femur neck fractures are intra-capsular fracture from the sub-capital region of the femur head to basi-cervical region of the femur neck. These fractures have a bimodal distribution and account for approximately 3.8% of fractures in adults, 50% of which occurring in the older population.[1] Majority of the femoral neck fractures in younger individuals are due to high-energy trauma such as sports injuries, car accidents, and fall from height while osteoporosis is one of the main risk factors for these fractures in elderly. Anatomical reduction, preservation of blood supply, and internal fixation is the treatment of choice for the femoral neck fractures, if not achieved adequately may lead to nonunion neck femur. According to Pauwels classification given in 1935, femoral neck fractures are divided into 3 types based on the Pauwels angle. Type I fractures, angle less than 30 degrees; type II, angle between 30-50 degrees ; fractures with Pauwel’s angle of 50°or more are classified into type III femoral neck fractures. Shearing forces and the component force of gravity are dominant in the Pauwels type III fracture. There is tendency of fracture displacement, varus collapse, malunion, nonunion and avascular necrosis of the femur head due to shearing forces in these fractures. When internal fixations is tried, they will generate not only compressive forces but also shearing forces. Hence, fixation strategy for the Pauwels type III fracture should resist the vertical shearing force as much as possible.[2], [3], [4] The most commonly used devices for fixation of vertical femoral neck fractures are multiple parallel screws in inverted triangle configuration or a sliding hip screw with or without an antirotation screw.[5], [6], [7] The principle of both techniques is fracture healing by sliding and compressing fragments when subjected to loading forces during weight-bearing. In Pauwels type III neck fracture, treated by ordinary cannulated cancellous screw fixation, shortening of the femoral neck, increased rate of non/malunion and femur head necrosis is often reported. Therefore, different fixation strategies with varying orientation of screws, with different insertion angles and/or association with locking plates, have been tried both in biomechanical models and patients.[8], [9], [10] There are reports which have shown good clinical outcome after reduction with a fixed-angle plate, but it requires an open reduction procedure, which is highly invasive, and the clinical results using a locking plate have not been encouraging.[8] A solution to these various increased rate of complications have been suggested by a new method of screw insertion called transverse cancellous lag screw fixation [TCLS] technique, in which a transverse lag screw is inserted from the lateral aspect of the greater trochanter intersecting fracture line at 90 degree angle. This construction offers a multiplane structure to lock the fracture ends and also compress fracture ends dynamically during the healing process. Also, due to transverse screw being placed at perpendicular to the fracture line there is optimum control of shear forces consequently avoiding the varus collapse, femur neck shortening, decreased rate of non-union and promote better union due to stable biomechanical construct. The rates of non-union/mal-union (6.7%), femur neck shortening (26.7%), and femur head necrosis (3.3%) are lower in this technique compared to inverted triangle configuration of cancellous screw fixation.[1], [2], [3], [4], [5], [6], [7], [8], [9], [10], [11] Considering the advantages of the TCLS fixation technique in Pauwels type III femoral neck fracture in young adults, we have analysed the functional and radiological outcome using fixation strategy with two parallel 7.0-mm lag cannulated cancellous screws inserted towards the neck at an angle similar to opposite hip neck – shaft angle (measured by templating), from the femoral shaft and a third transverse screw, inserted perpendicularly to the fracture line between the first two screws.
Materials and Methods
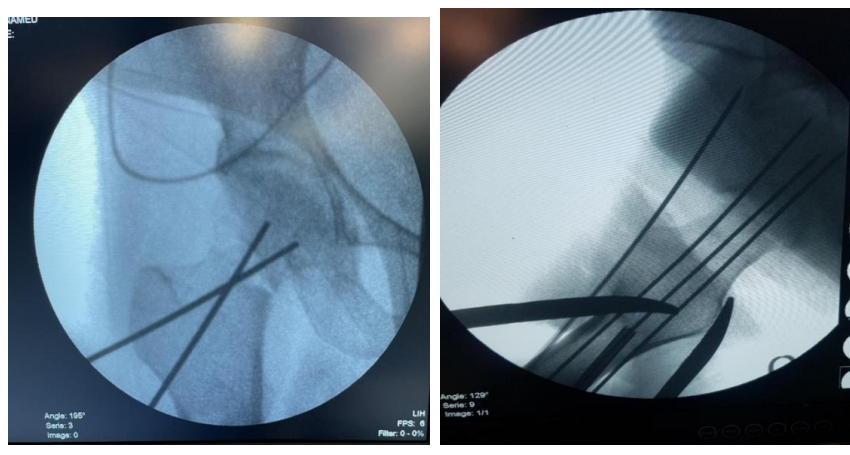
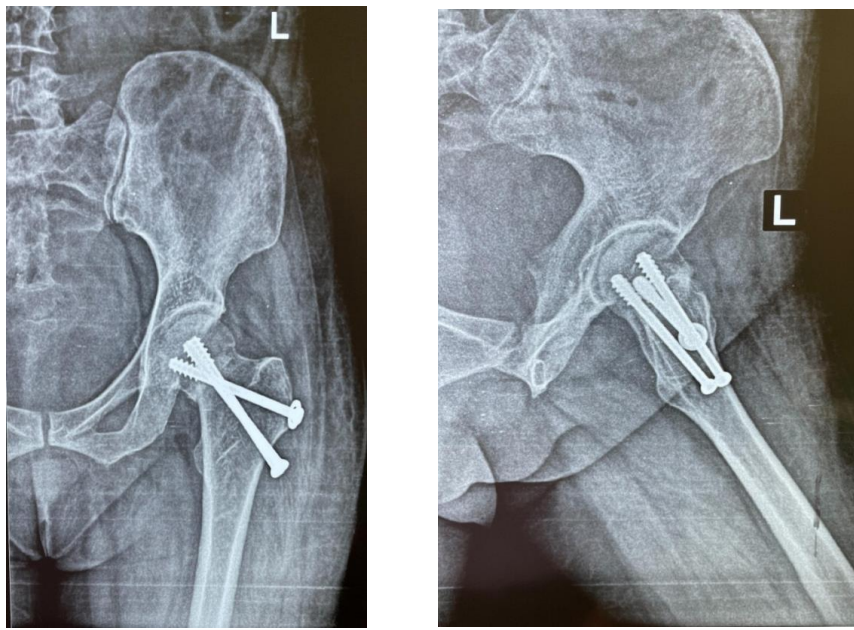
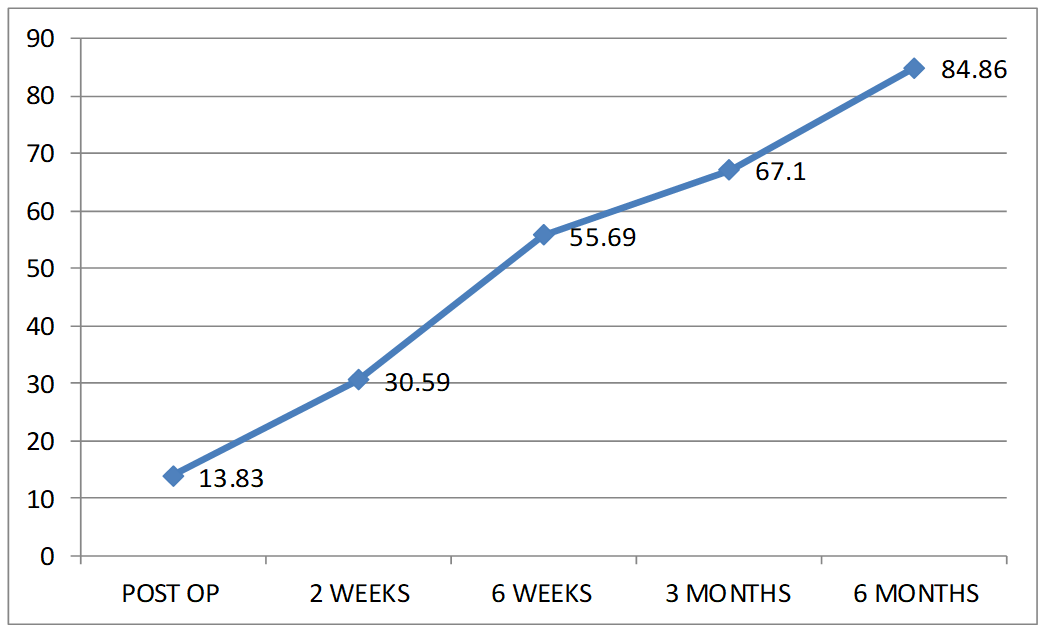
This is a prospective cohort study of 6 months duration on 29 patients, conducted in the department of orthopaedics, Deen Dayal Upadhyay Hospital, Hari Nagar, New Delhi. The inclusion criteria was Pauwels type III fracture neck of femur, Age group from 18-60 years of any gender and Patient presenting within 3 weeks of injury. Exclusion was done for Pathological fracture and any other associated fracture, advanced radiological osteoarthritis or rheumatoid arthritis in fractured hip, fracture neck of femur with dislocation of femoral head. After pre anaesthetic check-up patient was taken up for surgery on traction table. Closed reduction of the fracture was tried using Leadbetter or Whitmann’s method. In cases where anatomical reduction by closed method was not achieved then open reduction was done to reduce the fracture. After reduction painting and draping was done aseptically. A straight lateral incision, starting at the level of the lower end of the greater trochanter, with a distal length of 6–10 cm was given. Subcutaneous fat was dissected and tensor fascia lata was cut. Vastus lateralis was splitted and periosteum was elevated according to requirement. Reduction was secured with 2.0-mm guide wires. The guide wires were inserted according to the following sequence: the first guide wire was placed posteriorly in the femoral neck and the second was placed parallel to the first and anteriorly in the femoral neck. Both guide wire was inserted at an angle similar to opposite hip neck – shaft angle (measured by templating) from the femoral shaft, with an entry point slightly above the lesser trochanter from the lateral aspect of the femur. The third guide wire was placed centrally, inserted from the lateral aspect of the greater trochanter towards the central and lower part of the femoral head at a 90° angle from the fracture line, between the previously placed guide wires. Length of guide wires inside the bone was taken and then drilling was done over the guide wires. The 7 mm cannulated cancellous transverse screw with washer was placed first, followed by the posterior and anterior screws without washer. Next, we release the foot traction, and impacted the fracture with an additional tightening up of the screws. Final image was taken on image intensifier and if found satisfactory wound was closed and dressing was done. Wound was inspected on 2nd, 6th and 10th post-operative day and dressing was done. Patients were discharged depending on wound condition. Stitch removal was done at 2 weeks. Check X-ray and functional scoring was done at immediate post-operative period, 6 weeks, 3 months and 6 months. Range of motion exercises of hip and knee was started in immediate post-operative period, first passive then active as much as the patient was able to tolerate without discomfort. First 6 weeks patients were on strict non-weight bearing and subsequently partial weight bearing walk or toe touch walk was started for 8 weeks then full weight bearing was allowed. During the follow up examinations, the functional outcome was recorded by Harris hip score questionnaire and radiological outcome was documented by conventional radiographs by RUSH score and complication if any, was noted.
Results and Discussion
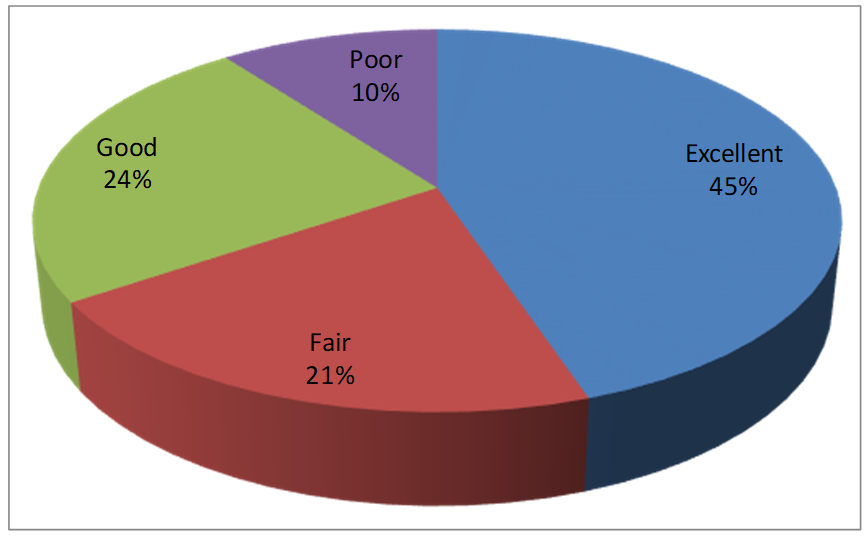
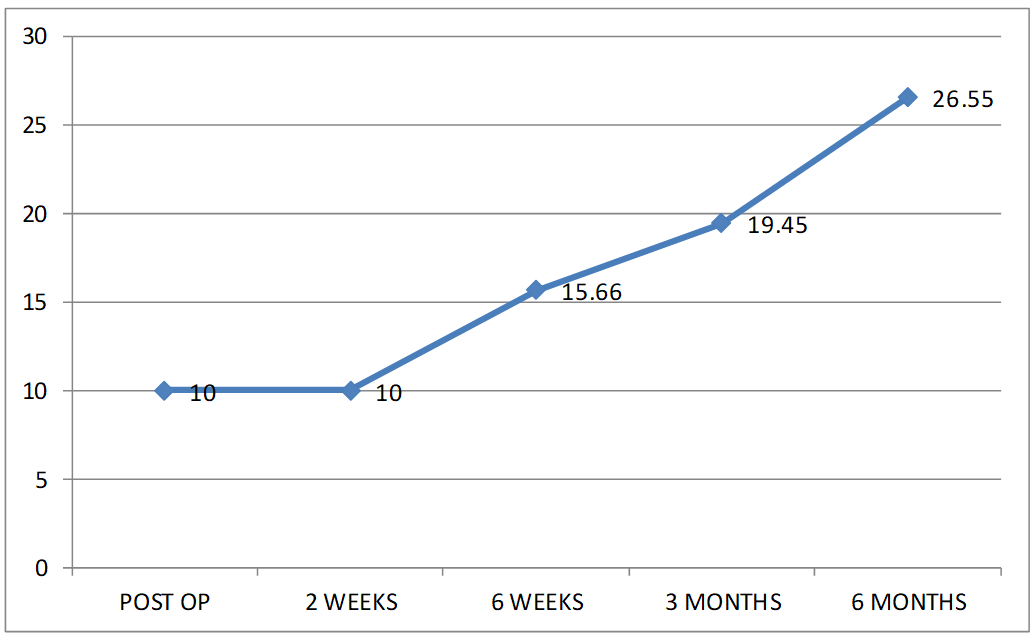
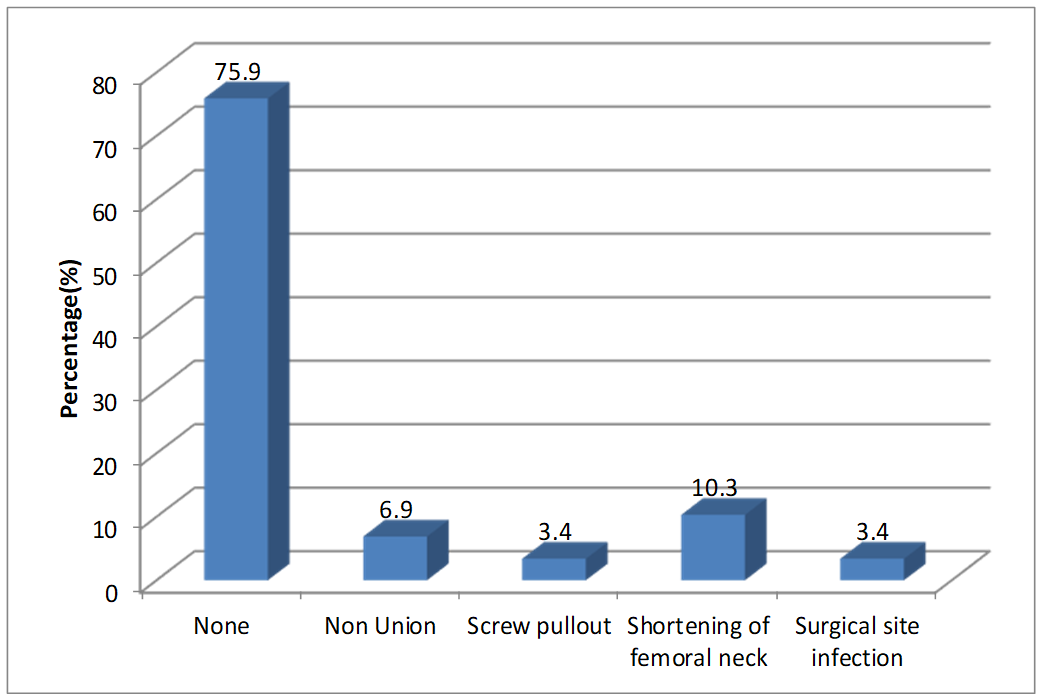
In our study, 13(44.8%) patients were having excellent functional outcome as assessed by Haris Hip Score, 7(24.1%) patients with good, 6(20.7%) patients with fair and remaining 3(10.3%) patients with poor functional outcome. There was significant statistical difference (p value < 0.05) between functional outcome and age. In the age group of less than or equal to 30 years, 100% patient had excellent functional outcome whereas in the age group of 51-60 years, 33% patients had excellent outcome, and 66.7 % had fair functional outcome. The mean RUSH score at 6 month follow up was 26.55. The union rate in the study was 93.10 % and the mean union time was 4 months. 3 patients developed shortening of femoral neck which may be due to dynamic compression during healing provided by the TCLS construct. None of our patient developed avascular necrosis. To know the actual rate of avascular necrosis, patients must be followed up for longer duration which was not possible in our study as the duration of our study was of 6 months only. Over all TCLS fixation technique had good results in our study. Firstly this construction not only improves the compression pressure, also offer a multi-plane structure to lock the fracture ends. Second, the addition of transverse lag screw (inserted perpendicularly to the fracture line) allows optimum control of shear forces in the fracture ends. Finally this transverse screw also provides rigid cortical support by transferring the bending moments from the femoral head and neck to the enhanced posterior lateral cortical support, which harmonized the function of the calcar femorale.
Conclusion
TCLS fixation method used in femoral neck fracture fixation has given good results in our study. Anatomical reduction is utmost important before fracture fixation. There may be difficulty in applying the transverse screw, but can be overcome by experience. By providing multiplane support, TCLS enhances fixation strength and gives excellent functional and radiological outcome.
Limitations
Bone densitometry could not be done to assess osteoporosis as this facility was not available in our hospital. Long term complications cannot be assessed due to shorter study duration of 6 months.
Source of Funding
None.
Conflict of Interest
None.
References
- Q Dong, Z Han, YG Zhang, X Sun, XL Ma. Comparison of Transverse Cancellous Lag Screw and Ordinary Cannulated Screw Fixations in Treatment of Vertical Femoral Neck Fractures. Orthop Surg 2019. [Google Scholar]
- M Shen, C Wang, H Chen, YF Rui, S Zhao. An update on the Pauwels classification. J Ortho Surg and Research 2016. [Google Scholar]
- RR Protzman, WE Burkhalter. Femoral-neck fractures in young adults. JBJS 1976. [Google Scholar]
- M Zlowodzki, O Ayieni, BA Petrisor, M Bhandari. Femoral neck shortening after fracture fixation with multiple cancellous screws: incidence and effect on function. J Trauma 2008. [Google Scholar]
- VT Selvan, MJ Oakley, A Rangan, MK Al-Lami. Optimum configuration of cannulated hip screws for the fixation of intracapsular hip fractures: a biomechanical study. Injury 2004. [Google Scholar]
- F A Bonnaire, A T Weber. Analysis of fracture gap changes, dynamic and static stability of different osteosynthetic procedures in the femoral neck. Injury 2002. [Google Scholar]
- A Enocson, LJ Lapidus. The vertical hip fracture - a treatment challenge: A cohort study with an up to 9year follow-up of 137 consecutive hips treated with sliding hip screw and antirotation screw. BMC Musculoskelet Disord 2012. [Google Scholar]
- PJ Nowotarski, B Ervin, B Weatherby, J Pettit, R Goulet, B Norris. Biomechanical analysis of a novel femoral neck locking plate for treatment of vertical shear Pauwel's type C femoral neck fractures. Injury 2012. [Google Scholar]
- MB Berkes, MT Little, LE Lazaro, RM Cymerman, DL Helfet, DG Lorich. Catastrophic failure after open reduction internal fixation of femoral neck fractures with a novel locking plate implant. J Orthop Trauma 2012. [Google Scholar]
- PJ Glassner, NC Tejwani. Failure of proximal femoral locking compression plate: a case series. J Orthop Trauma 2011. [Google Scholar]
- JAM Guimarães, LR Rocha, THN Rochaa, DC Bonfim, RS daCosta, ADS Cavalcanti. Vertical femoral neck fractures in young adults: a closed fixation strategy using a transverse cancellous lag screw. Injury 2017. [Google Scholar]