- Visibility 68 Views
- Downloads 15 Downloads
- DOI 10.18231/j.ijos.2023.006
-
CrossMark

Validity of percutaneous external fixator for calcaneal fractures to allow early weight bearing
Introduction
Calcaneum is the most common tarsal bone to fracture, accounting for about 60% of the tarsal bone fractures.[1] Among the calcaneal injuries, 60-75% of the fractures are of displaced intra-articular type.[2]
The people affected are mostly industrial workers and manual labourers who fall in the age group of 20 to 50 years who tend to fracture the calcaneum by falling from height during work, landing on the foot.[3] Most of the patients are the sole breadwinners of their family and hence their utmost priority is to return to their work as early as possible.
Generally, calcaneal fractures are treated either conservatively with a below-knee plaster or by surgical methods.[2] Surgical treatment commonly performed is open reduction and internal fixation of the fracture with plates and screws. But owing to the relatively poor blood supply and subcutaneous lie of the lateral surface of the calcaneum, there is high chances of infection.[3] Other surgical treatment methods including uniplanar, unilateral external fixation, Joshi’s external stabilization system have also been tried and documented.[3]
The controversy between operative and non-operative interventions remains ongoing since the surgical treatment methods possess a higher risk of infection, wound dehiscence, iatrogenic injury to the sural nerve and also require sophisticated infrastructure and implants.[3]
Furthermore, weight-bearing is not permitted for around 10 to 12 weeks in both conservative and surgical treatment methods.[2] Hence, apart from the physical agony, this situation causes a significant negative impact on the mental and economic condition of the patient’s family.[3]
In 2012, a study published by Vetrivel Chezian Sengodan described an innovative method of minimally invasive fixation of calcaneal fractures, which is superior to conservative management but eliminates the risks associated with open reduction and also allowed early weight bearing.[3]
We have analyzed the functional outcome of early weight-bearing with minimally invasive skeletal stabilization of calcaneal fractures in order to help the patients with early weight-bearing and early return to work.
Materials and Methods
This study was conducted at the Institute of Orthopaedics and Traumatology, Government Coimbatore Medical College Hospital, Coimbatore and Meenakshi Medical College Hospital and Research Institute, Kanchipuram, after obtaining ethical committee clearance. The study period was July 2019 to October 2021.
Fifteen patients in the age group of 20-65 years with 19 calcaneal fractures of less than 4 weeks duration were included in our study. Compound calcaneal fractures, avulsion fractures of the calcaneum and calcaneal fractures with skin blisters were also included.
The mode of injury was fall from height in 12 patients and road traffic accident in 3 patients. Unilateral calcaneal fracture was present in 11 patients and bilateral calcaneal fracture was present in 4 patients.
Among the 19 calcaneal fractures, 15 were closed fractures (78%) and 4 were compound fractures (22%). Among the 19 calcaneal fractures, 3 were extra-articular and 16 were intra-articular.
The procedure is performed under spinal anaesthesia, with the patient in supine position. Manual compression is given on either side of the calcaneum to restore the calcaneal height. The fracture fragments are palpated from the lateral subcutaneous aspect of the calcaneum. Three to four 1.8mm Kirschner wires are passed from the lateral to medial side, one in each major fragment. These Kirschner wires are interconnected using threaded rods and square nuts of the JESS fixator system to form a stable construct on both the medial and lateral sides ([Figure 1]).

Compression between the major fragments is achieved by reducing the distance between the K-wires passed through the respective fragments, before tightening the frame ([Figure 2]). To prevent loosening of the construct, these square nuts are tightened by the patient everyday under supervision using Allen key.
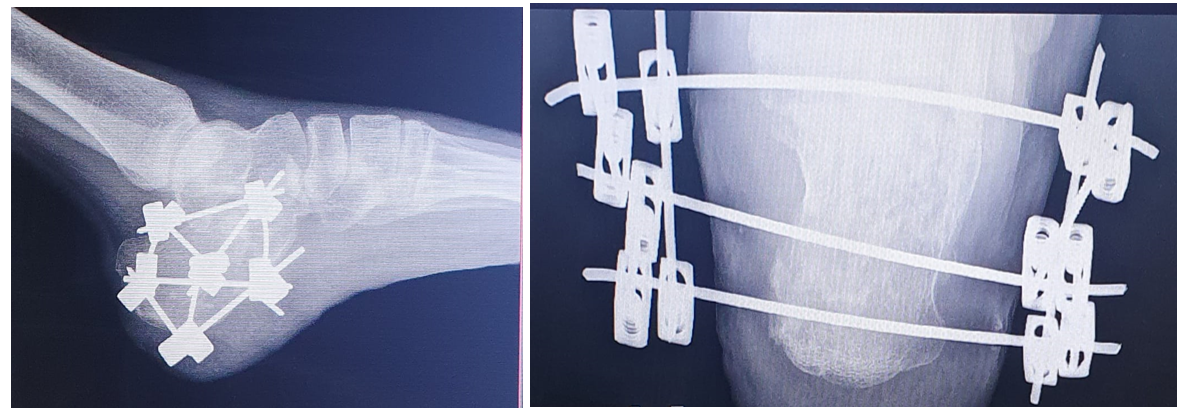
During the post-operative period, the patients are not immobilized with plaster of Paris. Patients are allowed for partial weight bearing on an average of 2 days and full weight bearing on an average of 12 days.
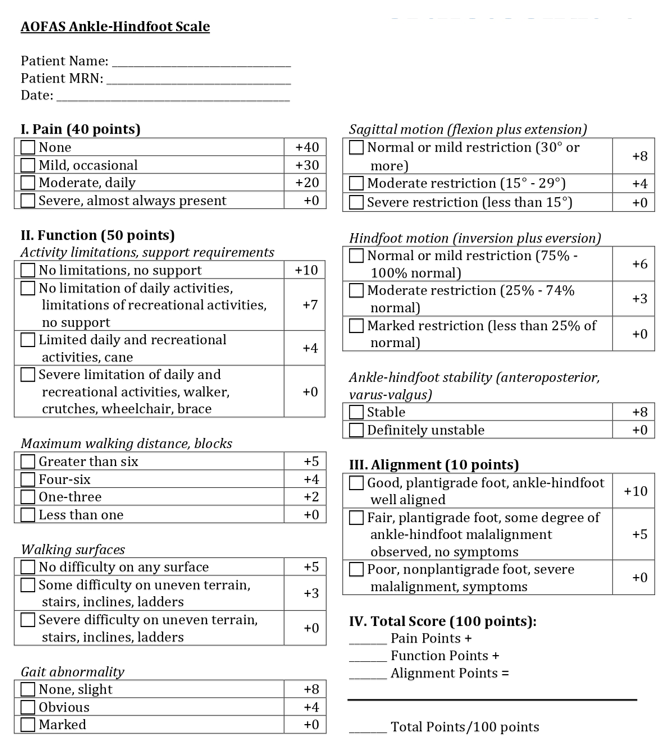
The patients are followed up at 4 weeks, 12 weeks ([Figure 3]) and 6 months and the final results are analyzed using the American Orthopaedic Foot and Ankle Society Score (AOFAS).

Results
The average time for surgery from the time of injury was 1.6 days. The mean time for partial weight-bearing was 2.72 days (range 1 to 6 days) and full weight-bearing was achieved at a mean of 11.7 days for unilateral calcaneal fractures (range 9 to 15 days) and a mean of 43.5 days for bilateral calcaneal fractures (40 to 49 days). Weight-bearing was delayed in patients with bilateral calcaneal fractures.
The patients were able to return to their original works in a mean of 35.6 days (range 24 to 52 days). Fracture union was achieved in all the 19 calcaneal fractures and the mean time was 52.63 days. The external fixator was removed at a mean of 56.57 days ([Table 1]). During the postoperative period, superficial pin site infection was present in 2 cases. Bone infection was not present in any cases. The average AOFAS score at 6 months follow-up was 86.15.
|
S.No |
Particulars |
Mean duration |
|
1 |
Injury to surgery time |
1.6 Days |
|
2 |
Partial weight-bearing |
2.72 Days |
|
3 |
Full weight-bearing |
U/L - 11.7 Days |
|
B/L – 43.5 Days |
||
|
4 |
Time to return to work |
35.6 Days |
|
5 |
Time for fracture union |
52.63 Days |
|
6 |
External fixator removal |
56.57 Days |
Discussion
Calcaneal injuries occur most commonly in younger male industrial workers in the age group of 20 and 40 years and mostly they are the sole breadwinners of their family. Hence, their foremost demand would be to return to their job as early as possible to support their family’s economic condition.[3]
With the long-standing debate of conservative or surgical management in calcaneal fractures, neither of them allows an early return to work and demand a non-weight bearing period of 10-12 weeks.[3]
Moreover, in open reduction and internal fixation of calcaneal fractures, complications like wound dehiscence, deep infection, osteomyelitis and injury to the sural nerve are common.[3]
As per the study conducted by Vetrivel Chezian Sengodan in 2012, the advantages of percutaneous skeletal stabilization for calcaneal fractures are: (a) Non scalpel approach hence minimal risk of wound infections. (b) It can be applied in compound calcaneal fractures, avulsion fractures and in cases with skin blisters without affecting the skin area. (c) Procedure can be done in any periphery centres as there is no need to have X-Ray/C-arm control in operating room and also the procedure is very cheap and cost effective when compared to the special reconstruction plates. (d) This method stabilizes the calcaneum alone and ankle is spared in contrast to the conservative method where ankle is immobilized using below-knee plaster. (e) It allows early-weight bearing and hence early return to work is possible.[3]
Our study also proves the advantages mentioned above with comparable results.
Buckley et al. in a randomized control trial found equal outcomes between operative and nonoperative treatment methods.[4]
Ibrahim et al. published a 15-year follow-up randomized control trial with 26 patients stating that the clinical outcomes were the same in operated and conservative cases.[5]
Agren et al. in a randomized control study comparing operative versus non-operative treatment for calcaneal fractures reported that operative treatment was not superior in managing displaced intra-articular calcaneal fractures at one year of follow-up but appeared to have some benefits at eight to twelve years, and the risk of complications was higher with operative treatment.[6]
In our study, intra-articular reduction is not attempted. Our aim is to maintain contact between the major fragments using a stable mini external fixator construct so as to facilitate bony union and to improve the functional outcome by early weight-bearing.[3]
The longer the patient remains out of work, the stronger is the negative impact of the economic condition of his family.[3] In our study, the mean duration for partial weight is 2.72 days and the mean duration for full weight-bearing is 11.7 days for unilateral calcaneal fractures and 43.5 days for bilateral calcaneal fractures. The mean duration to return to work is 35.6 days. During follow-up, the 6-month AOFAS score is 86.15 which is comparable to the score obtained by other modes of treatment published in the literature.[3]
Conclusion
Calcaneal fractures are common in our country due to fall from a tree or fall from height in industries. Most of the calcaneal fractures are treated by indigenous bonesetters in the rural parts of our country. In metros, it is treated by open reduction and internal fixation with plates and screws. In the case of plates and screws, the calcaneal plates are designed mostly as per the western population. Hence, the design and development of calcaneal plates for calcaneal fractures among Indians are slowly evolving. In the case of calcaneal fractures with blisters, surgery is deferred till the ‘wrinkle sign’ is positive. In compound calcaneal fractures internal fixation is mostly deferred. With internal fixation, early weight-bearing is not possible for 12 weeks till the fracture consolidates well.
Taking study published by Vetrivel Chezian Sengodan on 2012 as reference, in our study calcaneal fractures are fixed with mini external fixator percutaneously and it can be used in presence of compound fractures and with skin blisters. Though anatomical reduction cannot be attained completely weight bearing is possible from 2nd day after surgery and full weight bearing was possible in 2nd week.
The limitations of our study include a smaller number of cases. A large multi-centric study may be necessary to confirm our results.
Source of Funding
None.
Conflict of Interest
None.
References
- PJ Juliano, MS Myerson. Fractures of hind foot. Disorders of foot andankle 2000. [Google Scholar]
- RW Sanders, MP Clare, RW Bucholz, JW Heckman, CM Court-Brown, P Tornetta. Calcaneus fractures. Rockwood And Green's Fractures In Adults 2010. [Google Scholar]
- VC Sengodan, MM Sengodan. Early Weight-bearing Using Percutaneous External Fixator for Calcaneal Fracture. J Surg Tech Case Rep 2012. [Google Scholar]
- RE Buckley, RN Meek. Comparison of open versus closed reduction of intraarticular calcaneal fractures: a matched cohort in workmen. J Orthop Trauma 1992. [Google Scholar]
- T Ibrahim, M Rowsell, W Rennie, AR Brown, GJS Taylor, GPJ Taylor. Displaced intra-articular calcaneal fractures: 15-year follow-up of a randomised controlled trial of conservative versus operative treatment. Injury 2007. [Google Scholar]
- Å Per-Henrik, W Per, S Noor, S Arkan. Operative Versus Nonoperative Treatment of Displaced Intra-Articular Calcaneal Fractures. J Bone Jt Surg Am 2013. [Google Scholar]