Introduction
Intertrochanteric fractures can be treated with number of cephalomedullary implants available in market, i.e.; PFN TFN Long PFN ZNN Intertan nail Gamma nail PFNA2.All are devised to achieve painless, stable fixation and early mobilization. Hip fixation nail (HFN) designed by Author, is one of the single screw cephalomedullary nail for fixing stable as well as unstable trochanteric and peritrochanteric fractures of proximal femur and aimed at stable fixation and early ambulation. The pilot study of initial 43 cases and its clinical result is already documented and published earlier in September 2022 in Indian Journal of Orthopaedics Surgery.1
Hip fixation nail design
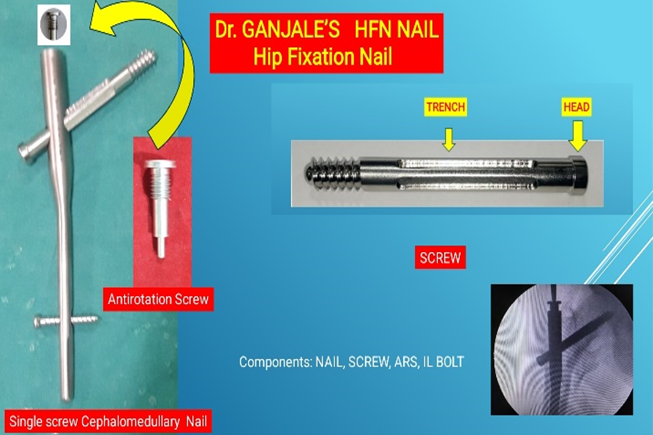
Hip Fixation Nail is single screw cephalomedullary implant for stabilizing intertrochanteric and peri trochanteric fractures.
Hip Fixation Nail comes in Regular sizes of 9 mm to 12 mm in diameter and a length of 18 cm Long HFN comes in length of 34 cm to 42 cm length with difference of 2 cm and is useful in intertrochanteric fractures associated with proximal shaft fractures and segmental fractures of femur (Figure 1, Figure 3).
The Proximal diameter of nail is 15mm, the mediolateral angulation is 5
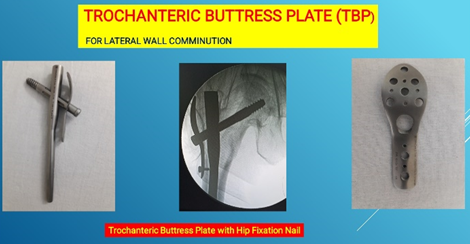
The nail has distal static as well as dynamic inter locking facility through jig. Hip fixation screw comes in 10.5mm diameter with tapering tip with deep threads for good bony purchase in the head and neck in young as well as in osteoporotic bones. It comes in sizes of 65mm to 110mm length with 5mm difference. The Screw has a head which rests on lateral wall after full tightening maintaining the compression. The screw has added advantage of maintaining compression which is achieved and is not dependent on sleeve or jig assembly. As the screw has head, Trochanteric buttress plate (Figure 2) can be added to this nail in case of lateral wall comminution. The shank portion of screw has four trenches on its surface to lodge the tip for Antirotation screw preventing the rotation and enhancing the rigid fixation. There is antirotation screw which is screwed from proximal end of nail, the tip of antirotation screw lodges on superior trench of screw, which prevents rotation of cervical screw and also acts as end cap for the nail. Interlocking bolts of 4.9mm are used to interlock distally in the HFN in static or dynamic mode.

Materials and Methods
A saw bone workshop was conducted during MOACON 2022 in September 2022.at Goa. A group of HFN workshop instructor’s orthopaedic colleagues was formed to demonstrate the technique of Hip Fixation Nail (HFN). The same group of orthopaedic surgeons and those colleagues who developed interest in performing HFN continued to operate and follow up their cases at their native practicing places. The study period was from January 2020 to May 2024. Trochanteric fractures were operated on fracture table.
Operative procedure
Hip fixation nail for trochanteric fractures was carried out under spinal anaesthesia on fracture table. Initial screening of reduction and alignment of fracture was assessed. Transfixation of fracture reduction was done with 2 thick k wires in unstable fractures. With a small incision Trochanteric entry was made with trochanteric entry awl designed by Dr Ganjale. The entry is just medial to tip Greater trochanter. Guide wire was passed through entry hole assessed in C arm. The entry was enlarged with starting reamer. Then Hip Fixation nail was passed over guide wire into femoral shaft canal .The hole in nail for cervical screw was aligned at neck level and maintaining anteversion, a guide wire was passed into neck through jig .The placement was checked under c arm for center center in AP and Lateral views or inferior in AP and a bit posterior in lateral view was confirmed. Graduated drills 5.5 mm and 8mm drill was used for drilling and screw placement. The correct sized cervical screw was selected and passed into neck till the screw tip had good subchondral purchase with TAD 10 mm. Distal IL was done through the jig. The jig was removed and antirotation screw was tightened at proximal end of HFN till it locked the cervical screw which is confirmed clinically with rotation of cervical screw with help of screw driver. If antirotation screw has properly locked the cervical screw, it should not rotate. Wound wash was given and closed with pressure bandage.
High subtrochanteric fractures with associated segmental shaft fractures were operated in lateral position using long hip fixation nail. Trochanteric buttress plate was used in cases of lateral wall fractures as per need. Distal interlocking was done by free hand technique under C arm.
Operated patients with stable fractures were mobilized early within two weeks period as per tolerance of patient with partial weight bearing to full weight bearing gradually with walker. Unstable fractures were mobilized at 6 weeks .Patients were followed up radiologically at six weeks intervals initially and later 3 months and six months. At every follow up patients were analyzed on radiological healing of fracture, any loosening or back out of implant, any infection. Clinical function like pain, limp, shortening, range of movement at operated hip, were recorded on a chart. They were followed up to one year. Few patients from initial pilot study who followed up during our study were also included in this multicentric study. Kyles Criteria (Table 2) was used to know the clinical and functional outcome. We also included HFN cases from our colleagues whose names are mentioned below have participated in this multicentric study on Hip Fixation Nail. The maximum period of follow up was 17 months and up to 24 months in few cases.
Table 1
Classification of trochanteric fracture depending on parts 2, parts 3, parts and 4 parts stable and unstable
Clinical cases representation
Following are the representative cases of Hip fixation nailing (case 1 to 7)
Case 1: Pre and immediate post operative images of a 68 year old male (Figure 4, Figure 5, Figure 6).
Case 2: 75 year old male patient sustained intertrochanteric fracture on right side (Figure 6).
Case 3: Case no 2 same patient sustained intertrochanteric fracture on left side after six months and was operated and fixed with Hip Fixation nail on left side and his follow up of both sides 30 months on right side and 24 months on left side (Figure 7).


Figure 6
Patient X–ray images A): Pre-operative images, B): post- operative x-ray and skin incision images
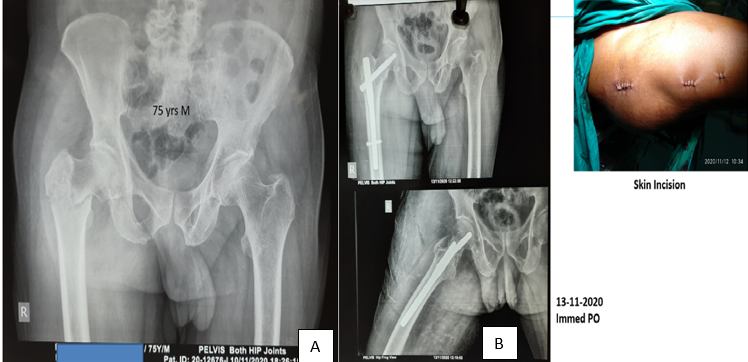
Figure 7
A): X-ray images of 6 months follow up right fracture healed well and fall again and sustained left intertrochanteric fracture , B):Right HFN 6 months post operative and Left HFN Immediately post operative, Left side immediately post operative X-ray, C): X-ray image after 30 months of operation, X-ray image after 24 months of operation.

Case 4: Communited unstable trochanteric fracture with vascular injury. (Figure 8).
Figure 8
A): Patient comminuted left trochanteric fracture with vascular injury, B): Image of x- ray immediate post operative showing HFN plus vascular repair, C): 2yrs follow uprecovery images, D): Clinical function images

Case 5: Hip fixation nail with trochanteric buttress plate (Figure 9 ).
Figure 9
A): Patient with associated head treated after remaining on ventilator 8 days, B): HFN plus TBP combo and Immediate post operative X-ray, C): X-ray image after 17 months followup

Case 6: Long hip fixation nail in 78 year old female (Figure 10,Figure 11).
Figure 10
A):Comminuted high subtrochanteric fracture left side, B):X- ray image of Immediate post operative closed long HFN, C):Image of skin incision
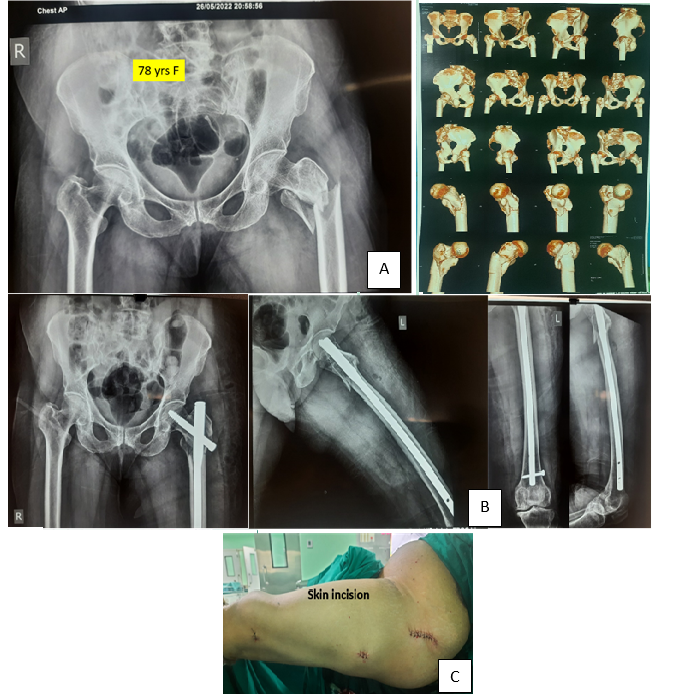
Figure 11
A):X–ray image after 7 weeks post operative, B):Patient image standing and walking after recovery, C):Follow up 14 months after surgery.

Case 7: Long hip fixation nail and trochanteric buttress plate in 70 yrs female with osteoporotic bone and thin lateral wall. (Figure 12)
Results
The results of the operated cases who have followed up atleast for one year and above were taken into consideration. The results of different orthopaedic colleagues were individually assessed by themselves of their own cases and were pooled in common results to have an average result. The final clinical outcomes were judged using Kyle’s criteria (Table 2). Post- operative xrays showed near anatomical fracture reduction in 87% of patient. There was a shortening of about one cm.to 1.5cms in 7 cases in comminuted trochanteric fractures associated with comminuted shaft fractures (Table 3).
Figure 12
X-ray image showing osteoporotic bone and thin lateral wall and Long HFN and trochanteric buttress plate.
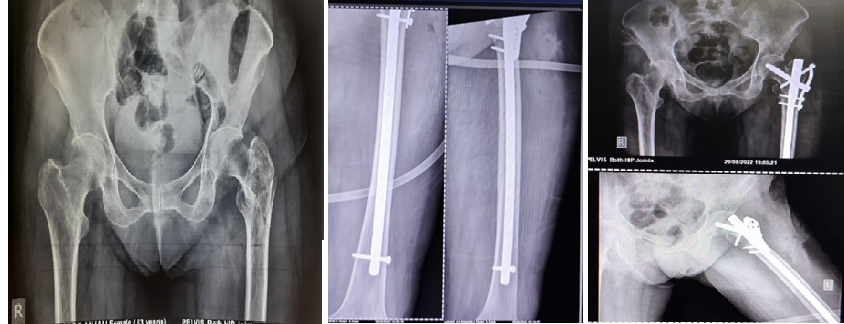
Table 2
Kyle’s criteria
The results showed 84.65% excellent results. 12.16 % Good results. 1.5% fair results and 1.5% poor results (Table 3).
Implant breakage 2 cases. Cervical screw breakage was due to inappropriate varus reduction and fixation in severely comminuted fracture, associated osteoporosis and patient incompliance. Cervical screw penetration in to joint 1 case .comminuted unstable, osteoporosis was the reason skin and subcutaneous infection in 4 cases which healed up with proper dressings antibiotic cover and wound care in 8 to 10 days.
Table 3
Number of cases operated by different orthopaedic surgeons and their results
Intra operative difficulties in getting anatomical reduction on fracture table due to comminution and inbeaking of neck in few cases were encountered and were addressed accordingly, but in five cases we had to accept some varus of neck due to inbeaking which could not be reduced well inspite of all maneauveres . But then they did well in post -operative follow up as they were advised nonweight bearing for initial 4 to 6 weeks and eventually united well.
Partial wedge effect was seen in 6 cases because of fragmented Greater trochanter and was displaced medial to nail.
Complication can and do occur in any surgical case with any implant fixation surgery. Many factors are determining the outcome, like type of fracture stable, unstable, comminution, quality of bone, age, type of implant, surgical skill and experience of operating surgeon, the adequate and optimum treatment, stability of fixation, general health of patient , cooperation of patient in post-operative period and many other intra operative technical difficulties encountered during surgery. The appropriate method and ideal implant for fixation of trochanteric and peritrochanteric fractures is the topic of debate with proponants and opponants each claiming advantages over the other methods.
Discussion
The aim of treating trochanteric fractures is to stabilize the bone by any fixation implant, make the patient painfree, mobilize early and make them self - dependent. The successful treatment of Trochanteric fractures depend on many factors like age, of patient fracture geometry like stable-unstable (Table 1), associated fractures, severity of comminution, quality of bone osteoporosis, time from fracture to treatment, adequacy of treatment, quality of reduction, type of implant fixation, surgical skill of operating surgeon, patient compliance and co-operation during post - operative period and general health of patient.2, 3
Richards Dynamic Hip screw is still most commonly used implant everywhere for its biomechanical properties like sliding and compression of fracture site and eventual healing in stable intertrochanteric fractures.4, 5, 6. This Hip Fixation nail works on same principles as of DHS and is intramedullary implant and load sharing implant . DHS is good implant for stable intertrochanteric fractures but is not good enough for fixing unstable trochanteric fractures and lateral wall comminutions. DHS requires a larger incision and exposure and handling of soft tissues which increases the morbidity with more chances of infection and blood loss. DHS being a surface implant where in the side plate has to be fixed with cortical screws to the shaft may weaken the bone especially in osteoporotic bones adding to stress risers and eventually fracture. The common causes of fixation failure is unstable fixation unstable fracture lack of anatomical reduction incorrect placement of DHS in neck.5, 3, 6. The mechanical causes are the abductor lever arm is more leading to varus stress. We all know intra medullary implants score over surface implants. The abductor lever arm is short in these intramedullary implants.4, 5, 7, 8.
There are numerous types of single screw or helical blade cephalomedullary nails available in market with some differences.
None of the single screw system in the market has head, they are headless screws or helical blades. The compression achieved on jig is by the resisting pull or push of aiming and compressing devices with sleeves resting on lateral wall of trochanter. The compression achieved on table with jig on is lost to some extent after disassembling the jig from nail. In case of PFNa2 the helical blade has to be hammered in which is surgeon dependent with what force he is applying. In attempt of hammering the blade can become loose and exchanging it makes loose fixation.9 So a screw system is better than blade system as screw can be gently screwed in manually achieving compression.
These implants demand mandatory compression for screw like 5mm 10mm etc. Many of the times this compression is not achieved or we cannot achieve because of fracture geometry. And we cannot limit our compression in between values (like 7mm, 12 mm etc) as recommended by companies, so the fixation is going to be unstable. Hip Fixation nail and screw system gives that freedom for achieving required optimal compression as per fracture geometry. The head of HFN screw rests against the lateral wall of trochanter and maintains the compression achieved till the end even after removal of jig. The HFN nail distal tip is bullet nose shaped and tapered to avoid stress risers at the tip of the nail .Now the newer HFN, proximal portion has flat lateral surface for easy gliding at entry site in the trochanter. Hip Fixation nail has a control of axial telescoping and rotational stability essential for unstable proximal femur fractures. The rotational stability is mainly due to Antirotation screw at the proximal end of nail locking the cervical screw and also allowing gradual sliding in dynamic locking mode. The cephalomedullary femoral reconstruction nails with a trochanteric entry point have gained the popularity in recent years. They have shown to be biomechanically stronger than extramedullary implants.5. The Gamma nail is associated with specific complications like broader proximal part of nail which is not suitable for Asian population and short statured females causing anterior thigh pain giving rise to stress risers in proximal shaft of femur at distal tip of nail.10, 6, 11 Intramedullary implants can withstand higher static and several fold higher cyclical loading than DHS type of implants. As a result the fracture heals without primary restoration of medial support.12 The implant temporarily compensates for the function of medial column. In A1 and A2 fractures axial loading leads to impaction of fracture. Whereas in A3 fractures this compression impaction does not occur and medial displacement of distal segment of fracture is commonly seen due to instability.13, 14, 15, 16
Conclusion
The results of HFN in treating stable and unstable trochanteric pertrochanteric and long HFN in subtrochanteric fractures of femur are promising and excellent. Hip Fixation nail has advantages of augmentation of fixation in comminuted fractures having facility of Trochanteric buttress plate and no other single screw with head system available in market is having this facility. Now the hip fixation screw has holes on its threaded portion for cement augmentation in cases of elderly osteoporotic bones. The screw system is better than helical blade system especially in elderly osteoporotic bones. The orthopaedic surgeons involved in this hip fixation study were happy and satisfied with surgeon friendly instrumentation and the simple procedure. Many new colleagues were convinced with Hip Fixation Nail. Hip fixation nail is an Indian make implant satisfies all the criteria of all cephalomedullary implants with added advantage for augmentation of fixation This surgery of Hip Fixation Nailing is very simple for new budding orthopaedic surgeons because of its surgeon friendly instrumentation and easy availability and is cost effective in urban and rural patients. Yet we need more number of cases to be operated to have a much happy results making it a happy fixation nail.
Acknowledgements
I would like to thank the following orthopaedic colleagues who believed in Hip Fixation Nail who actively and voluntarily shared their experience with clinical results in this study. Dr Vivek Potdar Ratnagiri, Dr Amol Shinde Akluj, Dr Pradeep Kothadia Solapur, Dr Swapnil Kothadia Solapur, Dr B. Shivashankar Solapur, Dr Sandeep Patil Karad, Dr Nitin Patil Karad, Dr Devendra Paliwal Nanded, Dr Nilendra Bhole Ratnagiri, Dr Niteen Deshpande Kolhapur, Dr Nagesh Naik Sangli , Dr Pradip Patil Kolhapur, Dr. Sameer Shaikh Miraj, Dr Neel Belsare, Dr Anand Karva Solapur, Dr Ajit Inamdar Waduj, Dr. Sanjeev Bhandari Solapur, Dr. Sanjay Dantkale Solapur, Dr Manmath Raut Solapur, Dr Rajan Dhandore Solapur, Dr Yash Shirshetty Solapur, Dr Sumit Mathpathi Solapur, Dr Jineshwar Kapale , Dr Sachin Kulkarni Solapur, Dr Milind Joshi Solapur, Dr Vijayanand Lokhande Pune.
My special regards and thanks to great teachers Dr V. M. Iyer sir, Dr D. D. Tanna sir and Dr Wasudeo Gadegone sir, for their inspirational blessings and appreciating the hip fixation nail.