Introduction
Periarthritis shoulder also called as Adhesive capsulitis or Frozen shoulder.1, 2, 3 The body creates excessive adhesion across the glenohumeral joint as a result of the idiopathic, chronic, and indolent degenerative process known as periarthritis shoulder, which causes discomfort, stiffness, and a reduction in range of motion.4, 5, 6, 3 It often appears between the ages of 40 and 70. In the general population, the prevalence of adhesive capsulitis is 3-55%, and it is 20% in those with diabetes.7, 8, 9 Many types of treatment have been employed in the treatment of shoulder disorder such as simple analgesia, NSAIDS, intraarticular steroid, platelet rich plasma injection and surgery.10, 11, 12, 13, 14, 15
Although this condition is associated with a number of risk factors, including female sex, trauma, age more than 40, thyroid disease,diabetes, stroke, myocardial infarction, extended mobility andt the existence of an autoimmune disease, the pathophysiology of this disorder is yet unknown.1, 16, 17, 18, 19
It's usual to think of adhesive capsulitis as having three phases. The first stage, known as "freezing," is characterised by escalating discomfort and stiffness that may last up to nine months.20, 21, 22, 23, 24, 25 The second stage, referred to as "frozen," entails a constant condition for a duration of four to twenty month.26 The third stage, known as "thawing," is a time of spontaneous healing that may last anywhere between five and twenty-six months.27, 5, 28, 29
Among the suggested therapies are, intra-articular corticosteroid, benign neglect and hyaluronic acid injections, physical therapy , deep heat modalities, oral corticosteroids, manipulation under anaesthesia, surgical release and hydrodilation.30, 31, 32, 33, 34 However, the best treatment option is a mater of debate. Due to its physiological effects,USG therapy is used as a treatment, which include, an increase in capillary permeability,increase in blood flow and tissue metabolism, an increase in pain threshold , an improvement in tissue extensibility, and a change in neuromuscular activity that cause relaxation of muscle.35, 36, 37, 38, 39
One of the methods often used to treat periarthritis of the shoulder is intra-articular corticosteroid injection.40, 41, 42, 43, 44, 45 In order to enhance and speed up tendon recovery, PRP has become a novel technique. 46, 47, 48, 49 It is thought to promote the soft tissue revascularisation and growth factors concentration increase. 50, 51, 33, 52 It is described as an autologous blood sample with platelet concentrations exceeding reference levels. 18, 53, 54, 55, 56
Numerous cytokines and growth like FGF,VEGF PDGF, TGF-beta, EGF, IGF-2, PDGF, and IGF-1, may be found in platelet rich plasma. 57, 58, 59 One of the newer methods of treating this very painful and in capacitating disorder uses keratinocyte growth factors and connective tissue growth factors. 60, 61, 62, 63 Several studies have shown its potential when compared to steroid injection and other forms of conservative therapy. 5, 64, 19, 65
PRP is more efficient and long-lasting than cortisone injection for the treatment of adhesive capsulitis, according to several research. 66, 67, 34
The main ideology behind this project is introduction of platelet rich plasma as a biological agent promoting healing when used in the treatment of periarthritis shoulder.
Aims and Objectives
To evaluate thes outcome of periarthritis shoulder treated with platelet rich plasma in the form of:
Materials and Methods
The research was done orthopaedic department of Narayana Medical College & Hospital, Nellore from November 2020 to June 2022 after getting ethical committee clearance.
Inclusion criteria
A total number of 30 patients in the age group of 35-60 years of either sex who are diagnosed with periarthritis shoulder for more than 4 weeks and not relieved by conservative treatment, patients with restricted active and passive movement at glenohumeral joint and patients giving informed consent for study were included in the study.
Exclusion criteria
Patients having chronic pain due to other causes like nerve damage or other neurological disorders, history of fracture around the shoulder joint, patients having local skin infection at the shoulder joint and patient not giving informed consent to be a part of study were excluded from the study and shoulderd pre procedure after 1 month, 3 months and at 6 months.
All the recorded data were interpreted statistically by paired t test and “p” value was calculated to conclude the thesis objectives statistically significant. The data was analyzed using paired t test. Then difference of pain relief between was statistically significant at both 3 months as well as 6 months follow up.
The ROM for Extension, abduction and flexion increased by an average of 12.7
In our study paired t test was employed to know the efficacy of PRP. Our study inferred that the pain relief was better with PRP at 6 months as compared to 1 month and pre procedure. So over a short term period the pain relief is better with PRP. The difference between pre procedure and 6 months after introducing platelet rich plasma was statistically significant as indicated by the “p” value.
Results
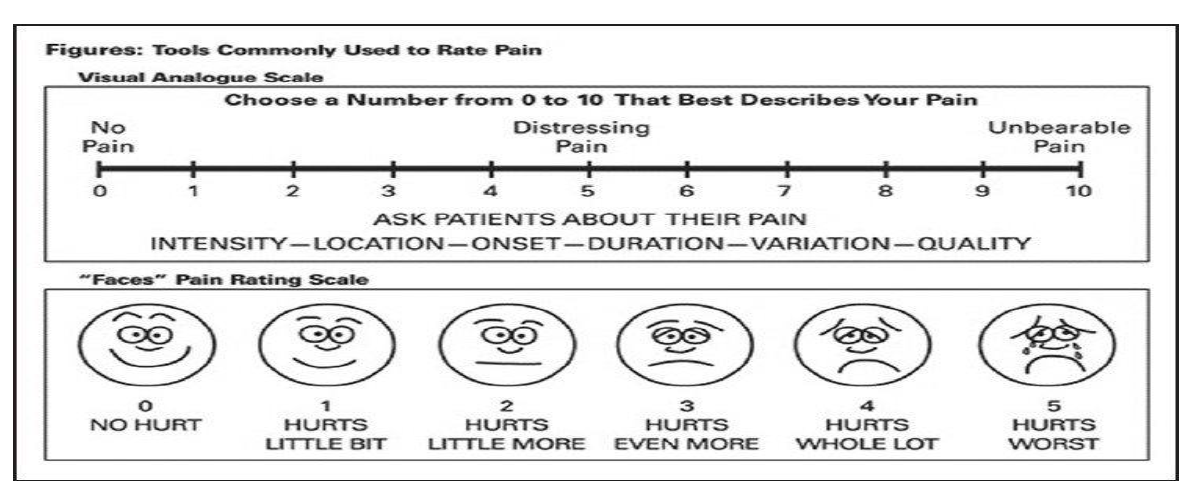
This study included 30 patients, participants were clinically evaluated, a baseline VAS scores, SPADI and ROM were recorded. Out of the 30 participants, 20 (66.66%) were males and 10 (33.33%) were females (Table 1).
Most of the patients i.e., 21 (70%) in our study were aged between 50-70 years with an average age 59.33 years (Table 2).
Table 2
Age distribution of patients studied
|
Age (i n years) |
Number of cases |
|
30-40 |
1 |
|
41-50 |
4 |
|
51-60 |
10 |
|
61-70 |
11 |
|
71-80 |
4 |
|
Total |
30 |
|
Mean ± SD |
59.33 |
The mean age was 59.33 years with standard deviation 14.79. The mean duration of the condition in all 30 patients suffering from Adhesive capsulitis was 15.167+10.268 months (Table 3).
Table 3
Duration (months) distribution in three groups of patients studied
Out of 30 participants 1 patient (3.33%) had transient hypotension, 1 (3.33) patient had nausea and 1 patient (3.33%) developed skin rashes along the upper limb after PRP injection (Table 4).
Table 4
Complication
|
Complication |
No. of cases |
|
Transient hypotension |
1 (3.33%) |
|
Nausea |
1 (3.33%) |
|
Skin rashes |
1 (3.33%) |
|
Total |
3 (10%) |
The mean VAS score at the presentation was 6.66+2.499. At 1 month these scores reduced to 5.866±1.408 has compared to baseline with p value of 0.131. At 3 months these scores reduced to 5.133±1.384 has compared to baseline with pvalue of 0.004. which is statistically significant. At 6 months these scores significantly reduced to 3.4±1.473 with p value of 0.0001 which is statistically significant (Table 5).
Table 5
Visual analouge scale mean, standard deviation and P value
|
Time Frame |
Mean |
Standard deviation |
P value |
|
Pre procedure |
6.66 |
2.499 |
|
|
1 months |
5.866 |
1.408 |
0.131 |
|
3 months |
5.133 |
1.384 |
0.004 |
|
6 months |
3.4 |
1.473 |
0.001 |
|
Total |
15.193 |
6.765 |
|
There was a statistically significant reduction inthe VASscore at 1month, 3months and 6months by paired t test.
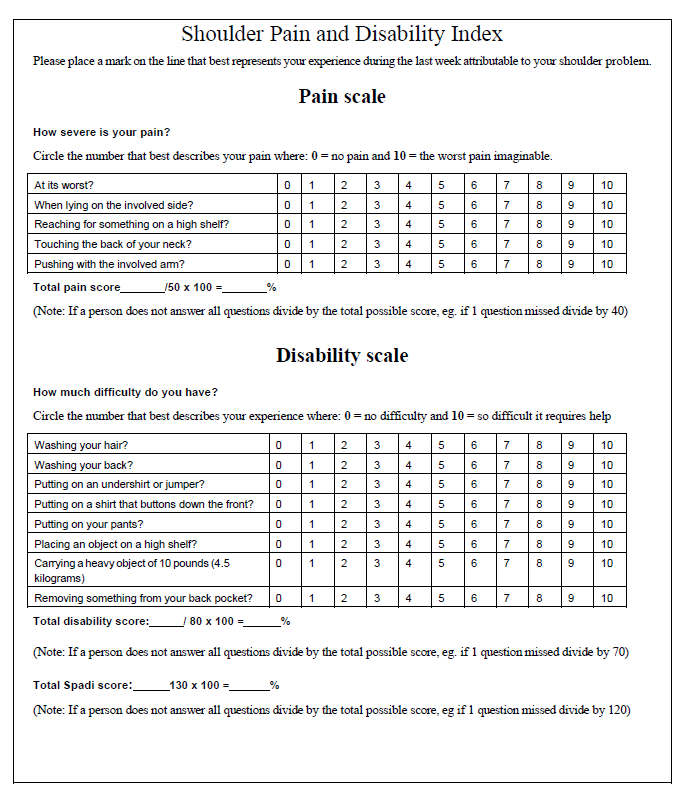
At 1 month SPADI score was 50.53±14.811 as compared to base line 43.0+14.857 with a p valuer of 0.0616 which is statistically not significant. At 3 months SPADI score was 59.43±14.441 as compared to base line with a value of 0.0001 which is statistically significant. At 6 months SPADI score was 74.76±10.926 as compared to base line with a p value of 0.0001 which is statistically significant (Table 6).
Table 6
Shoulder pain and disability index mean, standard deviation and P value
|
Time frame |
Mean |
Standard deviation |
P value |
|
Pre procedure |
43.3 |
14.857 |
|
|
1 months |
50.53 |
14.811 |
0.0616 |
|
3 months |
59.43 |
14.441 |
0.0001 |
|
6 months |
74.76 |
10.926 |
0.0001 |
|
Total |
177.49 |
55.025 |
|
After 6 months mean flexion was 116.33 ± 24.964 as compared to pre-procedure of 76
Table 7
Range of movements mean, standard deviation and P value
Discussion
Most of the patients ages were 40 to 70 years. The average age was 59.33±14.79 years. Kothari et.al., in their study observed that the mean age of all patients was 51.9+10.1 years.64
A minor male predominance was seen in this investigation. However, this distinction lacked statistical significance (P=0.825). Crubbs et.al., study showed adhesive capsulitis is more common in middle aged women than males.52
The mean duration of symptoms were 15.167+10.268 months. The mean duration of symptoms in all patients was 15.167±10.268 months, which was comparable to a study done by Calis et al., at Turkey in 2019 where mean symptom duration was 5.11±1.90.48
At presentation all the demographic and clinical variables in terms of SPADI, ROM in Extension, abduction, flexion was comparable between different follow up periods. At presentation the mean VAS scores was 6.66+4.99. The mean VAS score at the presentation was 66.66+2.499. At 1 month these scores reduced to 5.866±1.408 has compared to baseline with p value of 0.131. At 3 months these scores reduced to 5.133±1.384 has compared to baseline with p value of 0.004 which is statistically significant. At 6 months these scores significantly reduced to 3.4±1.473 with p value of 0.0001 which is statistically significant.
At 3 months follow up the mean VAS score decreased in the groups. Indicating improvement in patients symptoms subjectively. Further at 6 months the mean VAS score decreased very significantly.
The improvement in pain relief and decrease in VAS score in our study was comparable to a study done by Madhan jayaraman et al., at Davanagere in 2018,11 where it was determined that platelet rich plasma therapy is superior for adhesive capsulitis with 0.001 for VAS score and 0.01 for DASH score, which is statistically significant compared to hydro dissection, and the patients who received it showed improve drange of motion by the end of the first month of follow up.
32 patients who had intra-articular steroid injections for frozen shoulder as part of a research by Rawat et al.34 exhibited statistically significant pain alleviation after 12 weeks of follow-up. Shah carried out a research on 40 patients, and the results showed a substantial improvement in VAS and CSS ratings with a p-value of 0.05 after 3 doses of intra-articular steroid given at regular intervals. However, in contrast to prior trials, in our research a single dose of steroid injection was administered, and after 12 weeks, the steroid group saw statistically significant pain alleviation.
At 1 month SPADI score was 50.53±14.811 as compared to base line 43.0+14.857 with a p value of 0.0616 which is statistically not significant. At 3 months SPADI score was 59.43±14.441 as compared to base line with a p value of 0.0001 which is statistically significant. At 6 months SPADI score was 74.76±10.926 as compared to base line with a p value of 0.0001 which is statistically significant.
The improvement in SPADI scores in our study was comparable to the improvement in SPADI scores in the study done by Calis et al.,48 at Turkey which concluded when compared to baseline, there were substantial improvements in the SPADI pain, SPADI disability, and SPADI total scores in functional recovery (p<0.05).
At presentation mean extension was 18.6±7.486. At 1 month the extension improved to 21.66±8.097 with P value of 0.014 which is statistically significant. At 3 months the extension improved to 25.83±9.136 with P value of 0.0017 which is statistically significant. At 6 months the extension improved to 31.33±8.158 with P value of 0.0001 which is statistically significant.
At presentation mean abduction was 87.33±21.476. At 1 month the mean abduction improved to 97.66.±17.547 with P value of 0.0582 which is statistically significant. At 3 months the mean abduction improved to 10.1666±16.657 with P value of 0.00001 which is statistically significant. At 6 months the mean abduction improved to 126.833±18.325 with a P value of 0.0001 which is statistically significant.
At presentation mean flexion was 76±19.673. At 1 month the mean flexion improved to 86.16±21.043 with P value of 0.062 which is statistically significant. At 3 months the mean flexion improved to 100.6±22.757 with P value of 0.0003 which is statistically significant. At 6 months the mean flexion improved to 116.33±24.964 with a P value of 0.0001 which is statistically significant.
The ROM for extension abduction and flexion increased by an average of 12.7
Significantly more patients (92.50%) reported total pain relief after six months of follow-up. The current study outcomes were comparable to a similar study done by Kothari et al.,64 at Delhi in 2017, which concludes passive aswellas active range of motion of the shoulder, quick DASH, VAS and all showed statistically significant improvements after PRP treatment at 12 weeks compared to corticosteroid and ultrasonic therapy.
Conclusion
Hence we concluded that intra articular introduction of platelet rich plasma in periarthritis shoulder showed reduction in the intensity of pain, increase in angle of movements of shoulder joint and improvement in ability of carrying daily activities without restrictions which the patients were not able to do before.